Return to flip book view
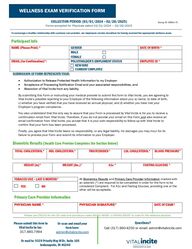
Message COLLECTION PERIOD: (03/01/2024 – 02/28/2025) Forms accepted for Physicals dated 03/01/2024 – 02/28/2025 Group ID: 00451-71 WELLNESS EXAM VERIFICATION FORM SUBMISSION OF FORM REPRESENTS YOUR: • Authorization to Release Protected Health Information to my Employer • Acceptance of Processing Notification Email and your associated responsibilities, and • Absolution of Vital Incite from any liability. By submitting this Form or instructing your medical provider to submit this form to Vital Incite, you are agreeing to Vital Incite’s possible reporting to your Employer of the following information about you: a) name, b) date of birth, c) whether you have verified that you have received an annual physical, and d) whether you have met your Employer’s program compliance. You also understand that the only way to assure that your Form is processed by Vital Incite is for you to receive a confirmation email from Vital Incite. Therefore, if you do not provide your email on this Form and also receive an email confirmation from Vital Incite, you accept that it is your sole responsibility to follow-up with Vital Incite to confirm that your form has been processed. Finally, you agree that Vital Incite bears no responsibility, or any legal liability, for damages you may incur for its failure to process your Form and submit its information to your Employer. Biometric Results (Health Care Provider Completes the Section Below) TOTAL CHOLESTEROL* HDL CHOLESTEROL* TRIGYCERIDES* LDL CHOLESTEROL* BLOOD PRESSURE* HEIGHT (in)* WEIGHT (lbs.)* A1c * FASTING GLUCOSE * TOBACCO USE – LAST 6 MONTHS* All Biometrics Results and Primary Care Provider Information marked with an asterisk (*) are required to be completed in order for the form to be considered Compliant. For A1c and Fasting Glucose, providing one or the other will be acceptable. YES NO Primary Care Provider Information PHYSICIAN NAME * PHYSICIAN SIGNATURE* DATE OF EXAM* Please use Z00.00 for the DX code and procedure codes 99381-99387 or 99391-99397 to code for the wellness physical. To encourage a healthy relationship with a primary care provider, our employees receive incentives for having received the appropriate wellness exam. Participant Info NAME (Please Print) * GENDER DATE OF BIRTH * MALE FEMALE EMAIL (for Confirmation)*: POLICYHOLDER’S EMPLOMENT STATUS EMPLOYEE ID * NEW HIRE CURRENT EMPLOYEE Please submit this form to Vital Incite by fax: 317.660.7994 Or scan and email your form here: admin@vitalincite.com Questions? Call (317) 660-4250 or email: admin@vitalincite.com Or mail to: 9339 Priority Way W Dr, Suite 105 Indianapolis, IN 46240